Polycystic Ovary Syndrome (PCOS) is one of the most common endocrine disorders affecting women of reproductive age, with a global prevalence ranging between 8% and 13%. For many women diagnosed with PCOS, the path to conception is hindered by ovulatory dysfunction. While lifestyle modifications and oral ovulation induction agents (like Letrozole) are the first line of defense, a significant number of patients eventually transition to Assisted Reproductive Technology (ART), specifically In Vitro Fertilization (IVF).
However, performing IVF for a patient with PCOS is fundamentally different from treating a patient with tubal factor infertility or diminished ovarian reserve. The “PCOS ovary” is hyper-responsive, unpredictable, and carries unique risks—most notably Ovarian Hyperstimulation Syndrome (OHSS).
At Prarambh IVF, we believe that success in PCOS-IVF cases lies in “Customized Controlled Stimulation.” This guide explores the strategic shifts required to turn the challenges of PCOS into a high-success IVF outcome.
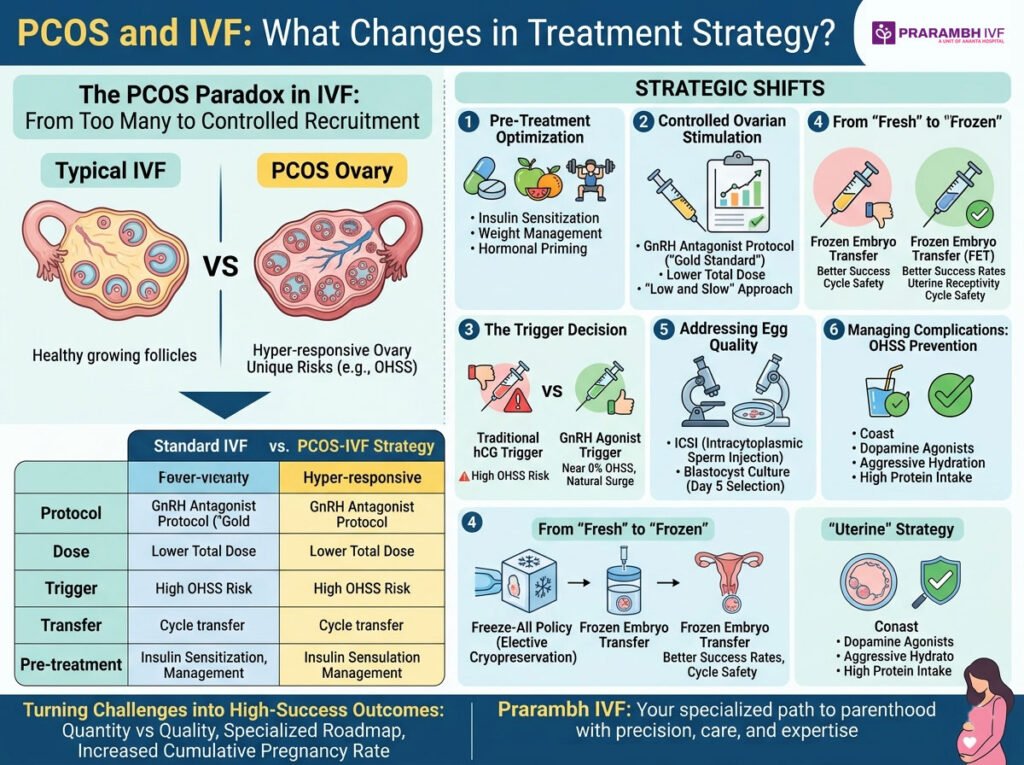
1. Understanding the PCOS Paradox in IVF
In IVF, we usually struggle to get enough eggs. In PCOS, the struggle is often having too many follicles of sub-optimal quality.
PCOS is characterized by an abundance of small, antral follicles. These follicles produce high levels of Anti-Müllerian Hormone (AMH), which inhibits the natural selection of a dominant follicle. When we introduce gonadotropins (injectable hormones) during IVF, these hundreds of “sleeping” follicles can all wake up at once.
The Strategic Shift: The goal changes from “recruiting as many follicles as possible” to “controlled recruitment and meticulous maturation.”
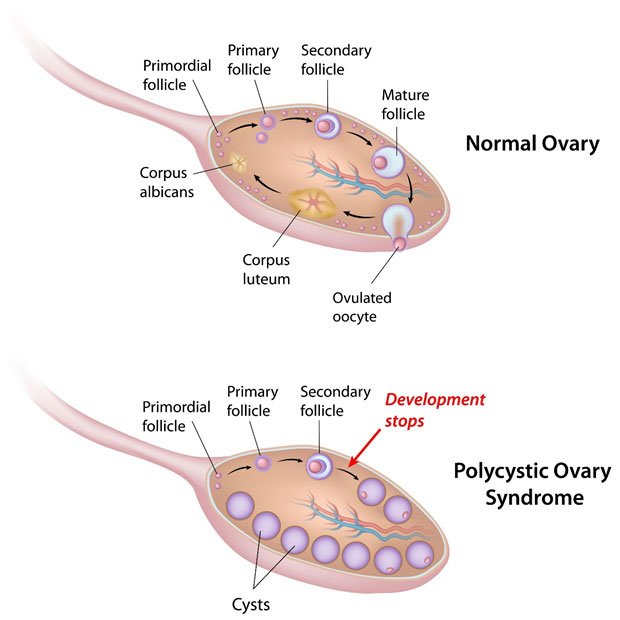
polycystic ovary syndrome
2. Pre-Treatment Optimization: The Foundation of Success
The IVF strategy for PCOS begins months before the first injection. At Prarambh IVF, we focus on three “Priming” pillars:
A. Insulin Sensitization
Hyperinsulinemia (high insulin levels) drives the ovaries to produce excess androgens (testosterone), which can impair egg quality.
- Strategy Change: The use of Metformin or Myo-inositol for 8–12 weeks prior to IVF. This improves insulin sensitivity, reduces androgen levels, and has been shown to decrease the risk of OHSS.
B. Weight Management and Lifestyle
A BMI over 30 can lead to higher gonadotropin requirements and lower implantation rates.
- Strategy Change: Even a 5-10% reduction in body weight can restore some hormonal balance, making the ovaries more responsive to lower doses of medication.
C. Hormonal Priming
- Strategy Change: Use of Oral Contraceptive Pills (OCPs) or Progestins in the cycle preceding IVF. This “quiets” the ovaries, prevents the formation of functional cysts, and allows for better synchronization of the follicle cohort.
3. Controlled Ovarian Stimulation (COS) Protocols
This is where the most significant technical shift occurs. Historically, the “Long Protocol” (using GnRH agonists) was the standard. Today, the GnRH Antagonist Protocol is the gold standard for PCOS.
Why the Antagonist Protocol?
In an Antagonist cycle, we start gonadotropins on Day 2 or 3 of the period and add a “blocker” (Antagonist) a few days later to prevent premature ovulation.
- Lower Total Dose: It requires fewer days of injections.
- Safety: It allows for the use of a “Lupron Trigger” (GnRH agonist trigger), which virtually eliminates the risk of life-threatening OHSS.
Dosage Strategy: “Low and Slow”
In a standard patient, a doctor might start with 225 IU of FSH. In a PCOS patient, we often start at 112.5 IU or 150 IU.
- The Logic: We want to coax the follicles to grow steadily. A “step-up” approach allows us to find the threshold dose without causing an explosive multi-follicular response.
4. The “Trigger” Decision: The Game Changer
In a traditional IVF cycle, Human Chorionic Gonadotropin (hCG) is used as the “trigger” shot to finalize egg maturation. However, in PCOS, hCG acts like fuel on a fire, significantly increasing the risk of OHSS because it stays in the system for days.
The Strategic Shift: The GnRH Agonist Trigger
By using an agonist (like Leuprolide) instead of hCG:
- The body releases its own natural surge of LH and FSH.
- The hormonal stimulus clears from the body quickly.
- Result: The risk of severe OHSS drops from ~10-15% to nearly 0%.
5. From “Fresh” to “Frozen”: The “Freeze-All” Policy
One of the most profound changes in PCOS treatment strategy is the move away from fresh embryo transfers.
In a PCOS cycle, the high estrogen levels caused by numerous follicles make the uterine lining (endometrium) “over-mature” and less receptive to an embryo. Furthermore, if a patient gets pregnant during a fresh transfer in a high-response cycle, the natural hCG produced by the pregnancy can trigger “late-onset OHSS,” which is dangerous.
The Strategic Shift: Elective Cryopreservation
At Prarambh IVF, we frequently recommend:
- Egg Collection & ICSI.
- Freezing all viable embryos (Vitrifaction).
- Waiting 1-2 months for the patient’s hormones to return to baseline.
- Frozen Embryo Transfer (FET): Transferring the embryo into a “natural” or mildly prepared uterus.
Studies show that for PCOS patients, FET success rates are significantly higher than fresh transfer rates.
6. Addressing Egg Quality: The Role of the Embryology Lab
It is a common myth that PCOS means “poor egg quality.” In reality, the issue is often the “microenvironment” of the follicle. High androgens and insulin can lead to eggs that are “cytoplasmically immature.”
Strategic Adjustments in the Lab:
- ICSI (Intracytoplasmic Sperm Injection): Because PCOS eggs can sometimes have thicker outer shells (zona pellucida), ICSI ensures fertilization by injecting a single sperm directly into the egg.
- In Vitro Maturation (IVM): In extreme cases where stimulation is too risky, we can collect immature eggs and mature them in the lab. While less common than standard IVF, it is a specialized tool in the PCOS arsenal.
- Blastocyst Culture: Growing embryos to Day 5 (Blastocyst) helps us filter out those that may have genetic or developmental lags due to the PCOS environment.
7. Managing Complications: Ovarian Hyperstimulation Syndrome (OHSS)
OHSS is the “shadow” that follows PCOS treatment. It involves fluid leaking into the abdominal cavity, causing bloating, pain, and in severe cases, kidney or lung issues.
Strategic Prevention:
- Coast: If estrogen levels get too high, we may stop gonadotropins for a few days before the trigger (coasting).
- Dopamine Agonists: Starting Cabergoline on the day of the trigger to reduce vascular permeability.
- Aggressive Hydration: High protein intake and electrolyte-rich fluids post-retrieval.
8. The Psychological Component: Managing Expectations
PCOS patients often feel a sense of “failure” when their cycles are delayed (due to freeze-all) or when they have 20 eggs but only 3 high-quality embryos.
Strategic Communication:
At Prarambh IVF, we prioritize counseling. We educate patients that in PCOS, Quantity ≠ Quality. Our goal is not the highest number of eggs, but the healthiest baby. Understanding that a “Freeze-All” strategy is a safety and success optimization—not a setback—is vital for patient mental health.
9. PCOS and Pregnancy: The Journey Continues
The strategy doesn’t end at a positive pregnancy test. PCOS patients have a higher risk of:
- Gestational Diabetes (GDM)
- Pregnancy-Induced Hypertension
- Pre-term labor
The Strategic Shift: Integration of high-risk obstetric care early on. We continue Metformin therapy in many cases through the first trimester and implement strict glucose monitoring.
10. Summary: The Prarambh IVF Approach
To summarize, the treatment of PCOS within an IVF framework has moved from a “one size fits all” to a “safety-first, precision-based” model.
| Feature | Standard IVF | PCOS-IVF Strategy |
| Stimulation Protocol | Often Long Agonist | GnRH Antagonist |
| Starting Dose | Standard (225 IU) | Low Dose (112.5 – 150 IU) |
| Trigger Type | hCG | GnRH Agonist (Lupron) |
| Transfer Strategy | Fresh Transfer | Freeze-All (FET) |
| Pre-treatment | Minimal | Metformin / Inositol / OCPs |
Conclusion
PCOS presents a unique set of hurdles, but with the right strategic shifts, it also offers a unique advantage: an abundance of opportunities. Because PCOS patients typically have a high ovarian reserve, their cumulative pregnancy rate (the chance of pregnancy across all embryos created from one egg retrieval) is among the highest in the field of infertility.
At Prarambh IVF, we don’t see PCOS as a barrier; we see it as a condition that requires a specialized roadmap. By prioritizing insulin sensitivity, utilizing antagonist protocols, employing the agonist trigger, and embracing frozen embryo transfers, we transform the “PCOS Paradox” into a successful path to parenthood.
If you have been struggling with PCOS and are considering IVF, remember that the strategy makes the difference. Your journey starts here—with precision, care, and expertise.
For a personalized consultation regarding PCOS and IVF, visit us at Prarambh IVF.