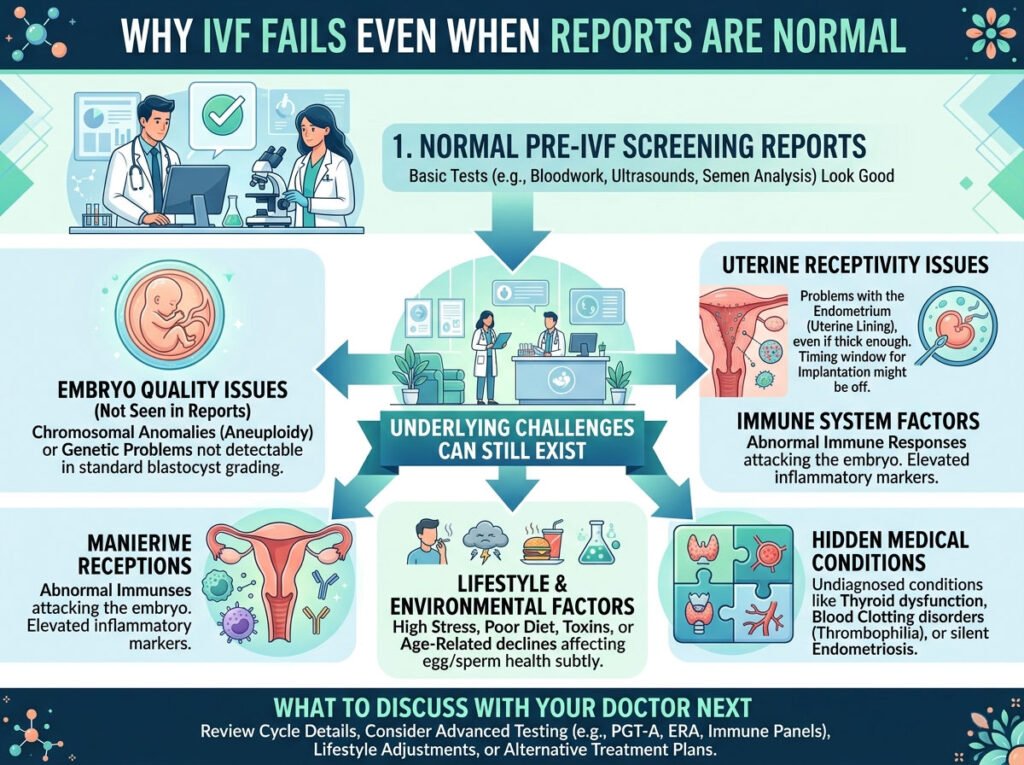
Establishing a successful pregnancy through In Vitro Fertilization (IVF) is a complex biological journey. For many couples, the most frustrating experience is a failed cycle when all preliminary tests—blood work, ultrasounds, and semen analysis—suggested a high probability of success. When “on paper” everything looks perfect, a negative result feels inexplicable.
However, “normal reports” usually refer to standard diagnostic parameters, which often only scratch the surface of reproductive biology. Below is a comprehensive analysis of why IVF cycles may fail despite normal clinical reports.
1. The “Black Box” of Embryo Quality
Standard IVF reports typically grade embryos based on morphology (how they look under a microscope). While an embryo may be graded as “4AA” (excellent), looks can be deceiving.
Chromosomal Abnormalities (Aneuploidy)
The most common reason for IVF failure is genetic. Even in young, healthy couples, a significant percentage of embryos are aneuploid (having the wrong number of chromosomes). Standard reports do not show this unless Preimplantation Genetic Testing for Aneuploidy (PGT-A) is performed. An embryo can look “perfect” morphologically but be genetically incapable of resulting in a live birth.
Metabolic and Mitochondrial Health
The “battery” of the embryo resides in the mitochondria. If the egg’s mitochondria lack the energy to drive the rapid cell division required after implantation, the embryo will stop developing. This “energy failure” is not visible in standard blood tests or basic embryo grading.
2. Endometrial Receptivity: The “Window” Problem
Even the healthiest embryo cannot implant if the “soil” (the uterine lining) is not ready.
The Window of Implantation (WOI)
In most women, the lining is receptive to an embryo during a specific 24-to-48-hour window. However, about 25–30% of women have a “shifted” window—meaning their lining is ready earlier or later than average. If the embryo transfer is performed outside this precise window, the cycle will fail despite a “normal” looking lining on an ultrasound.
Displaced Microbiome
Recent research highlights the importance of the uterine microbiome. A “normal” report confirms the thickness of the lining, but it doesn’t always account for chronic endometritis (a silent inflammation) or a lack of healthy Lactobacillus bacteria. An unbalanced uterine environment can trigger an immune response that rejects the embryo.
3. Silent Pathologies Not Caught in Standard Screens
Standard fertility workups often look for major issues like blocked tubes or large fibroids. However, subtle issues can remain hidden.
- Adenomyosis: This occurs when endometrial tissue grows into the muscular wall of the uterus. It can be missed on standard ultrasounds but significantly impacts implantation rates.
- Hydrosalpinx: Sometimes a fallopian tube is blocked and filled with fluid. This fluid can leak back into the uterus, acting as a toxin to the embryo. If the blockage is subtle, it might not appear on a basic scan.
- Endometriosis: Even “silent” endometriosis can affect egg quality and the inflammatory environment of the pelvis, even if reports show regular ovulation.
4. The Male Factor: Beyond the Count and Motility
A “normal” Semen Analysis (SA) measures volume, count, and movement. However, it says very little about the “cargo” inside the sperm.
DNA Fragmentation
High levels of Sperm DNA Fragmentation (SDF) mean the genetic material is damaged. Sperm with high fragmentation can still fertilize an egg, but the resulting embryo often stops growing around day 3 or fails to implant. Standard reports rarely include an SDF test unless specifically requested.
Oxidative Stress
Environmental factors, heat, or lifestyle can cause oxidative stress in semen, damaging the sperm membrane and DNA, which standard motility tests might miss.
5. The Immune System Interference
The body’s immune system is designed to attack “foreign” objects. Since an embryo contains 50% DNA from the father, the mother’s immune system must actively “tolerate” it.
In some cases, the immune system overreacts. Natural Killer (NK) cells or certain antibodies (like those found in Antiphospholipid Syndrome) may attack the developing placenta or cause tiny blood clots that prevent the embryo from establishing a blood supply. These immunological factors are rarely part of a “normal” initial fertility screen.
6. Lifestyle and Epigenetic Factors
While your clinical reports measure hormones and anatomy, they don’t measure the cellular environment.
- Chronic Stress: High cortisol levels can affect blood flow to the uterus.
- Systemic Inflammation: Diets high in processed sugars or undiagnosed food sensitivities can keep the body in a pro-inflammatory state, making the uterus less “hospitable.”
- Environmental Toxins: Exposure to endocrine disruptors (BPA, phthalates) can affect the “cross-talk” between the embryo and the uterus at a molecular level.
Moving Forward: What to do After a Failed Cycle?
If you have experienced a failure despite normal reports, it is time to dig deeper. At Prarambh IVF, we specialize in “unexplained” failures by looking beyond the basics:
- Advanced Embryology: Utilizing Blastocyst culture and considering PGT-A for genetic screening.
- Uterine Evaluation: Utilizing Hysteroscopy or the ERA (Endometrial Receptivity Array) to find the exact window of implantation.
- Male Factor Depth: Testing for DNA fragmentation.
- Tailored Protocols: Adjusting medication types and timing to suit your unique biological rhythm.
A failed cycle is not the end of the road; it is a piece of diagnostic information that helps us refine the strategy for the next attempt.
For a personalized consultation and to review your previous cycles, visit us at Prarambh IVF. We believe in turning “unexplained” into “understood.”