What is Embryo Grading & Why It Matters in IVF: A Comprehensive Guide
For many couples embarking on an In-Vitro Fertilization (IVF) journey, the laboratory phase can feel like a “black box.” Among the most technical yet vital aspects of this process is embryo grading. At Prarambh IVF, we believe that an informed patient is a confident patient. Understanding how your embryos are graded can help you manage expectations and participate more actively in decisions regarding your fertility treatment.
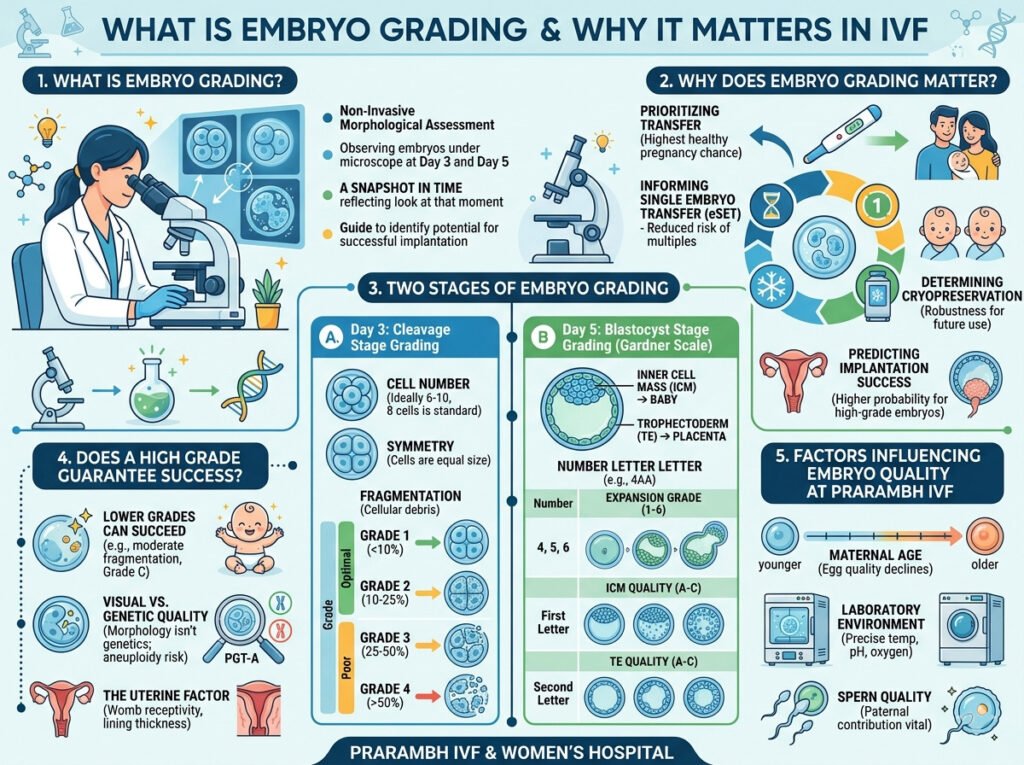
1. What is Embryo Grading?
Embryo grading is a non-invasive morphological assessment tool used by embryologists to evaluate the quality and developmental potential of an embryo (New Hope Fertility Center, 2026). It involves observing the embryo under a high-powered microscope at specific time points—typically on Day 3 and Day 5—to assess its appearance, cell division, and structure (Genesis Fertility, 2026).
It is important to understand that grading is a snapshot in time. It reflects how an embryo looks at that specific moment, providing a guide for which embryos are most likely to implant successfully in the uterus (ARC® Fertility, n.d.).
2. Why Does Embryo Grading Matter?
Embryo grading is not just about “ranking” embryos; it serves several critical clinical functions:
- Prioritizing Transfer: It helps specialists identify which embryo has the highest statistical probability of resulting in a healthy pregnancy (Birla Fertility, n.d.).
- Informing Single Embryo Transfer (eSET): By identifying high-quality embryos, clinics can confidently recommend transferring one embryo at a time, which significantly reduces the risks associated with multiple pregnancies (twins or triplets) (Gardner et al., 2004).
- Determining Cryopreservation: Grading helps decide which embryos are robust enough to survive the freezing (vitrification) and thawing process for future use (Genesis Fertility, 2026).
- Predicting Implantation Success: While not a guarantee, research shows that higher-grade embryos generally have higher implantation rates compared to lower-grade ones (IVF Resources, 2025).
3. The Two Stages of Embryo Grading
Embryos are typically graded at two distinct stages: the Cleavage Stage (Day 3) and the Blastocyst Stage (Day 5/6). Because the embryo changes fundamentally between these days, different grading systems are used for each.
A. Day 3: Cleavage Stage Grading
On Day 3, the embryo’s cells (called blastomeres) are dividing, but the embryo itself is not yet growing in size (ARC® Fertility, n.d.).
- Cell Number: A healthy Day 3 embryo typically has between 6 and 10 cells. Eight cells is often considered the “gold standard” for this stage (Genesis Fertility, 2026).
- Symmetry: Ideally, the cells should be of equal size. Uneven cell sizes can sometimes indicate underlying developmental issues.
- Fragmentation: This refers to small bits of cellular debris that break off during division. Fragmentation is graded on a scale:
- Grade 1: <10% fragmentation (Optimal).
- Grade 2: 10–25% fragmentation.
- Grade 3: 25–50% fragmentation.
- Grade 4: >50% fragmentation (Poor) (ARC® Fertility, n.d.).
B. Day 5: Blastocyst Stage Grading (The Gardner Scale)
By Day 5, the embryo has reached the Blastocyst stage, consisting of 70–120 cells. It now contains two distinct cell types: the Inner Cell Mass (ICM), which becomes the baby, and the Trophectoderm (TE), which becomes the placenta (IVF Resources, 2025).
The Gardner Grading System uses a number followed by two letters (e.g., 4AA):
- Expansion Grade (Number 1–6): Measures how much the embryo has expanded and if it has begun to “hatch” from its outer shell (the zona pellucida).
- Grade 4: Fully expanded.
- Grade 5: Starting to hatch.
- Grade 6: Fully hatched (IVF Resources, 2025).
- Inner Cell Mass Quality (First Letter A–C):
- A: Many cells, tightly packed.
- B: Several cells, loosely grouped.
- C: Very few cells (ARC® Fertility, n.d.).
- Trophectoderm Quality (Second Letter A–C):
- A: Many cells forming a cohesive layer.
- B: Fewer cells, irregular layer.
- C: Very few cells (New Hope Fertility Center, 2026).
4. Does a High Grade Guarantee Success?
It is a common misconception that only “AA” graded embryos lead to babies. While a “4AA” embryo has a high statistical chance of success, embryo grading is subjective and limited.
- Lower Grades Can Succeed: Many “Grade C” embryos or Day 3 embryos with moderate fragmentation have resulted in perfectly healthy pregnancies (Genesis Fertility, 2026).
- Visual vs. Genetic Quality: Grading only assesses appearance (morphology). An embryo may look “perfect” (4AA) but have chromosomal abnormalities (aneuploidy). This is why some patients opt for Preimplantation Genetic Testing (PGT-A) alongside traditional grading (Divine Women’s Hospital, n.d.).
- The Uterine Factor: Even the highest-grade embryo cannot implant if the uterine environment is not receptive or if there are issues with the lining (Birla Fertility, n.d.).
5. Factors Influencing Embryo Quality at Prarambh IVF
At Prarambh IVF, we utilize advanced laboratory protocols to maximize embryo quality:
- Maternal Age: Egg quality naturally declines with age, which can impact embryo grading (Pramukh IVF Center, n.d.).
- Laboratory Environment: Our state-of-the-art incubators maintain precise temperature, pH, and oxygen levels to mimic the human fallopian tube and uterus.
- Sperm Quality: The paternal genetic contribution is equally vital for healthy embryo development.
Conclusion: Science Meets Hope
Embryo grading is a powerful tool that helps us navigate the complexities of IVF. It provides a roadmap for selection, but it does not define the final outcome. Every embryo represents a unique possibility.
If you are undergoing treatment at Prarambh IVF & Women’s Hospital, our embryology team will provide you with a detailed report of your embryo development. We encourage you to discuss these grades with your specialist to understand the best path forward for your specific journey.